Putting the ‘value’ in value-based payments
Putting the ‘value’ in value-based payments matthew holt

By JOSH SEIDMAN
Like Matthew Holt, I have also been ranting about the fact that “We’re spending way too much money on stuff that is the wrong thing.” As Matthew said, “it’s a rant, but a rant with a point!” And that’s a lot better than most rants these days. In addition to having a point, I’m also bringing a lot of data to my rant.
More specifically, we’ve known for a long time that clinical care only drives 20% (maybe less) of health outcomes, yet we continue to spend more and more on it.
We do that despite the well-documented fact that the U.S. performs worse than most OECD countries despite spending far more. I remember, in my first health care job in 1990, being blown away that the U.S. spent $719 billion on health care (or $1.395 trillion in 2022 dollars). Here we are, trillions of dollars later ($4.465 trillion) doing the same thing and expecting a different result.
After more than 30 years in health CARE, I decided that I really wanted to start doing something about HEALTH, which is why 3 years ago I joined Fountain House, the founder of the clubhouse movement, a psychosocial rehabilitation model for people with serious mental illness (SMI)—a model now replicated by 200 U.S. clubhouses and another 100+ in more than 30 countries around the world. It was actually people living with SMI that launched Fountain House in 1948, realizing long ago that addressing social drivers of health offered a new road to recovery and rehabilitation. Now 75 years later, we’re finally seeing some parts of the health care system come to terms with the necessity of addressing health-related social needs.
With decades of evidence behind us, Fountain House has spent the last year and a half building an economic model to understand clubhouses’ societal economic impact when one takes into account a wide range of costs—mental health, physical health, disability, criminal justice, and productivity or lost wages.
The net impact for the average person served by clubhouses is more than $11,000 per year—and twice that amount for someone with schizophrenia. (We also know that clubhouses have a huge impact on quality of life, agency, self-esteem, and many other important aspects associated with recovery and rehabilitation—which is personally much more important to me, just not the subject of my current rant.)
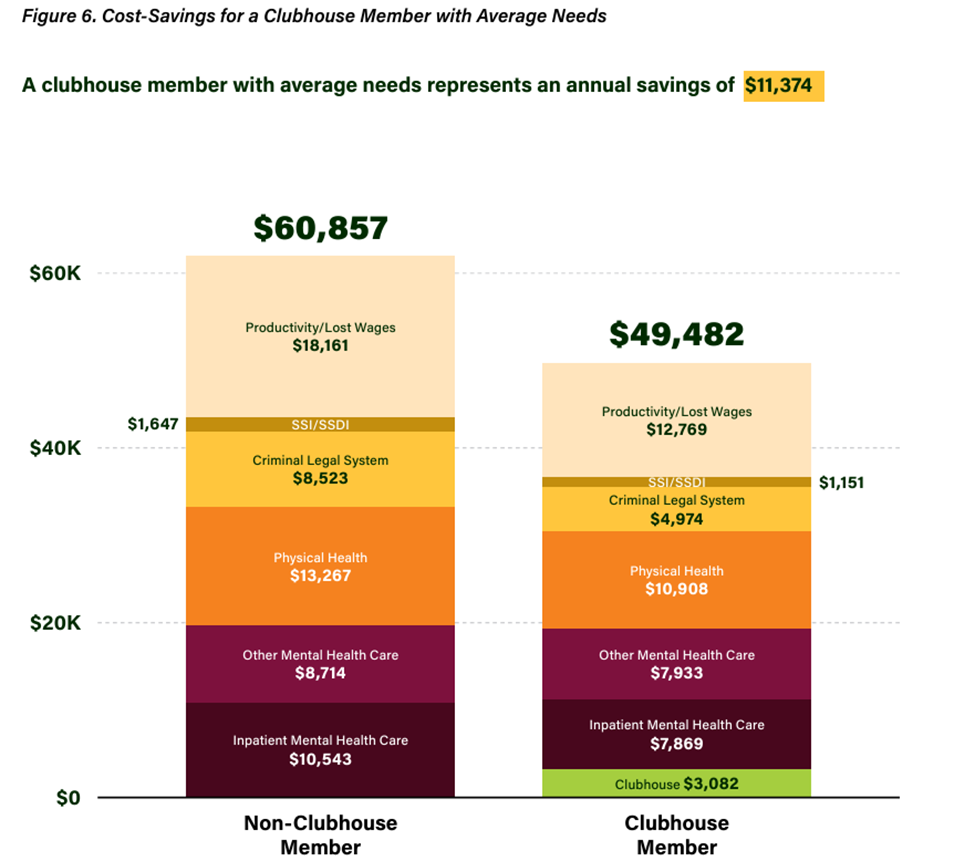

The medical costs alone are dramatic and, interestingly, it’s a fairly even balance between mental and physical costs. Importantly, for the average clubhouse member, the social costs outweigh the medical cost benefits.
U.S. clubhouses currently serve approximately 60,000 people. That’s a tiny fraction of the more than 15 million people in the U.S. living with SMI. If we could even support 5% of them with clubhouses, an extrapolation of our model suggests that would generate more than $8.5 billion per year in savings to the public, not to mention dramatically changing the life trajectories for so many people.
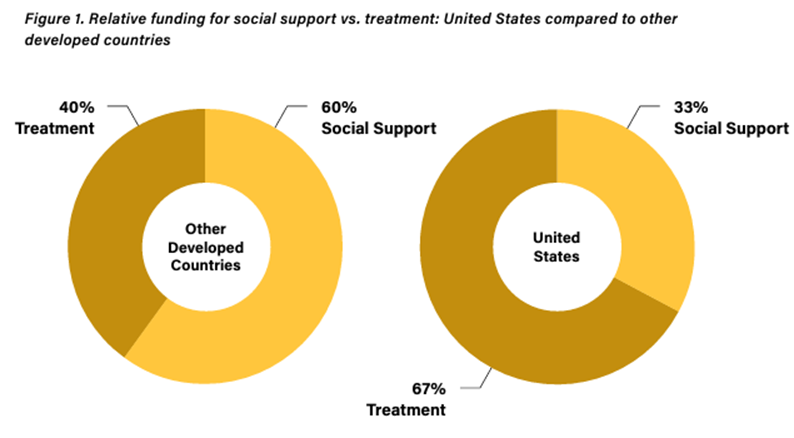
The broader point here is that we don’t have to make the choices we do from a societal perspective. If you compare the U.S. to other developed countries, you notice a complete flip in emphasis on social support versus clinical care.
Given that it’s unlikely that we’re going to suddenly dramatically shift the balance of resources in the U.S., we need to find new ways to encourage a greater emphasis on addressing health-related social needs. As we push toward new value-based payment models, we need to find ways to reward performance for achieving social outcomes (e.g., employment levels, educational attainment, housing stability) as well as the patient-reported outcomes (e.g., quality of life, loneliness reduction) that we know contribute greatly to recovery and rehabilitation.
Joshua Seidman, PhD, is Chief Research and Knowledge Officer for Fountain House, a national mental health nonprofit working for and alongside people with serious mental illness to support their recovery.